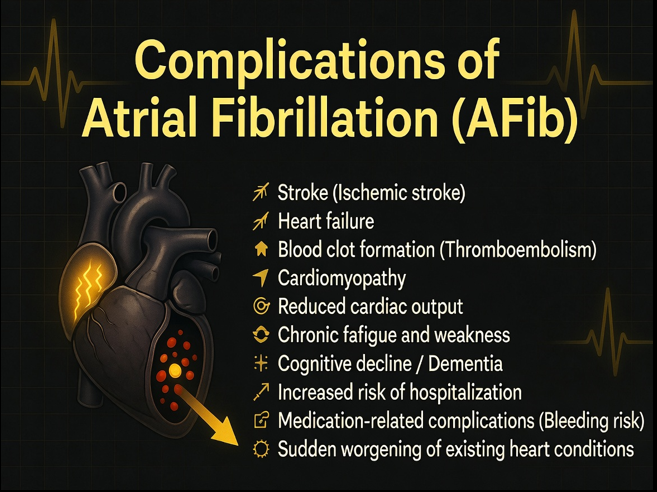
Atrial fibrillation is an irregular heartbeat, or arrhythmia. Atrial fibrillation also known as AFib or AF, caused by chaotic electrical signals in the heart’s upper chambers (atria), can lead to blood clots, stroke, heart failure and other heart-related complications. AFib is the most common type of irregular heart rhythm.
Description: Irregular and often rapid heart rhythm originating in the atria.
Characteristics: ECG Rhythm with absence of distinct P-waves, irregular R-R intervals.
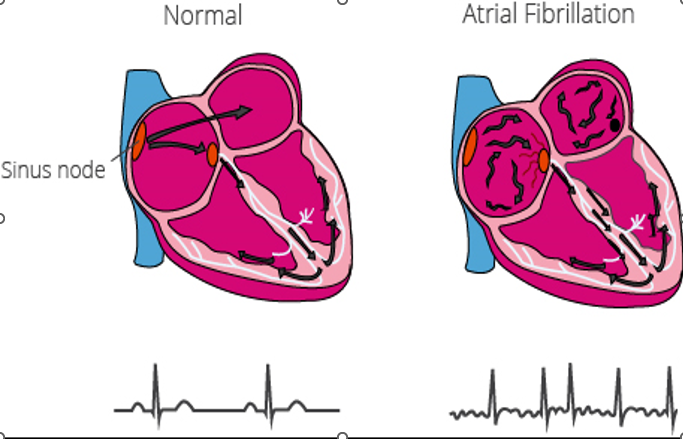
Normal Heart Rhythm vs Atrial Fibrillation
A NORMAL HEART RHYTHM is a coordinated heartbeat (60–100 bpm) initiated by the SA node,
while Atrial Fibrillation (AFib) is a chaotic, irregular, and often rapid arrhythmia originating from multiple sites in the atria, causing them to quiver.
Pathophysiology of Atrial Fibrillation
Rapid and disorganized electrical activity occurs in the atria
Electrical impulses originate from ectopic foci (pulmonary veins) instead of the SA node
Leads to ineffective atrial contraction (atria quiver, not pump properly)
Results in reduced cardiac output
AV node receives chaotic signals and transmits them irregularly
Causes irregularly irregular ventricular rhythm
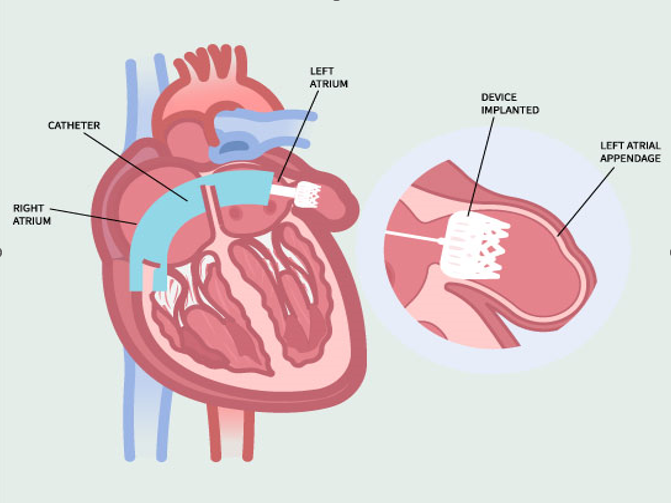
Ineffective contraction leads to blood stasis, especially in the left atrial appendage
Increases risk of thrombus (clot) formation
Clots may embolize → can cause stroke
Long-term AF leads to atrial remodeling (dilation and fibrosis)
Four Main Types Of Atrial Fibrillation
(Afib)
1. Paroxysmal AFib
Episodes start suddenly and stop on their own
Usually lasts less than 7 days (often < 24 hours)
Heart returns to normal rhythm without treatment
Symptoms may come and go (palpitations, dizziness)
2. Persistent AFib
Lasts more than 7 days
Does not stop on its own
Requires treatment (medications or cardioversion) to restore normal rhythm
3. Long-Standing Persistent AFib
Continuous AFib lasting more than 12 months
Rhythm control becomes more difficult
Often associated with structural changes in the atria
4. Permanent AFib
AFib is accepted as ongoing
No further attempts to restore normal rhythm
Focus is on:
Rate control
Anticoagulation (to prevent stroke)
Clinical Symptoms of Atrial Fibrillation (AFib)
Palpitations
Fatigue Or Weakness
Shortness Of Breath (Dyspnea)
Dizziness
Chest Pain Or Discomfort
Reduced Exercise Capacity
Fainting (Syncope
Diagnosis of Atrial Fibrillation (AFib)
Electrocardiogram: Irregular rhythm and absence of P waves.
Holter monitoring: 24–48 hours or longer.
Echocardiography (2D Echo):Assesses heart structure, valve disease, and atrial enlargement.
Chest X-ray : Helps evaluate heart size and lung conditions contributing to AFib.
Blood tests : Includes thyroid function tests (TSH), electrolytes, and renal function.
Atrial Fibrillation (AFib) Management
Control heart rate: Maintain a safe ventricular rate to improve cardiac output.
Restore and maintain normal rhythm (sinus rhythm) :convert irregular rhythm to normal.
Prevent thromboembolism (stroke prevention):Reduce risk of clot formation.
Improve symptoms and quality of life: Reduce palpitations, fatigue, and breathlessness.
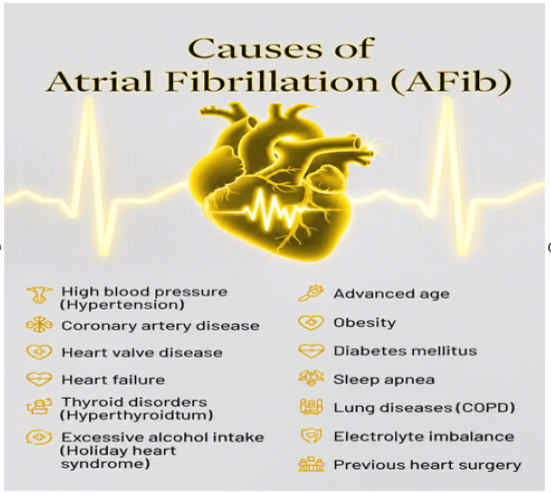
Treat underlying causes:Manage conditions like hypertension, thyroid disorders, or heart disease.
Nursing Interventions
Monitor vital signs (HR, BP, SpO₂) frequently.
Assess ECG rhythm continuously.
Symptom Assessment in which we evaluate for palpitations, chest discomfort, and shortness of breath.
Administer prescribed medications (beta-blockers, calcium channel blockers, digoxin).
INR Monitoring if the patient is on warfarin and heparin.
Monitor for signs of bleeding (gums, urine, stool, bruising).
Patient Position in semi-Fowler’s position to improve cardiac output.
Monitor signs of reduced perfusion (fatigue, hypotension, altered mental status).
Assess neurological status regularly (speech, limb strength, consciousness).